Unprecedented Advances Fuel Progress in the Treatment of AL Amyloidosis
Light-chain amyloidosis is a rare plasma cell disorder that involves the production of a misfolded amyloidogenic light chain by a plasma cell clone that deposits in various organs leading to organ failure. Traditionally, the treatment paradigm has focused on eliminating the culprit plasma cell clone with autologous hematopoietic cell transplantation (AHCT) in eligible patients or with bortezomib (V; Velcade)-based therapy (typically in combination with cyclophosphamide and dexamethasone [VCd]) in AHCT-ineligible patients. The goal of therapy for patients with AL amyloidosis is to achieve a swift and deep hematologic response which correlates with survival and organ function improvement.1
Therapeutic efforts have pivoted on implementing novel strategies that generate the deepest hematologic response, as well as targeting amyloid fibrils for immune destruction by means of antiamyloid monoclonal antibodies in the hopes of reversing organ dysfunction.
Andromea Opens the Door
Daratumumab (Dara; Darzalex) is a human IgG1k anti-CD38 monoclonal antibody that is approved for the treatment of newly diagnosed and relapsed multiple myeloma. CD38 is abundantly expressed on plasma cells in patients with AL amyloidosis drawing attention to Dara as an attractive therapeutic means. Dara showed significant efficacy in small case series in relapsed AL amyloidosis with response rates of 70% to 80%.2,3 The pivotal phase 3 ANDROMEDA study (NCT03201965) assessed the effect of the addition of Dara to the standard of care VCd in patients with newly diagnosed AL amyloidosis.4 The study enrolled all patients with AL amyloidosis except for those with advanced Mayo 2004 stage IIIB patients (troponin ≥ 0.035 mcg/L and NT-proBNP ≥ 8500 ng/L).
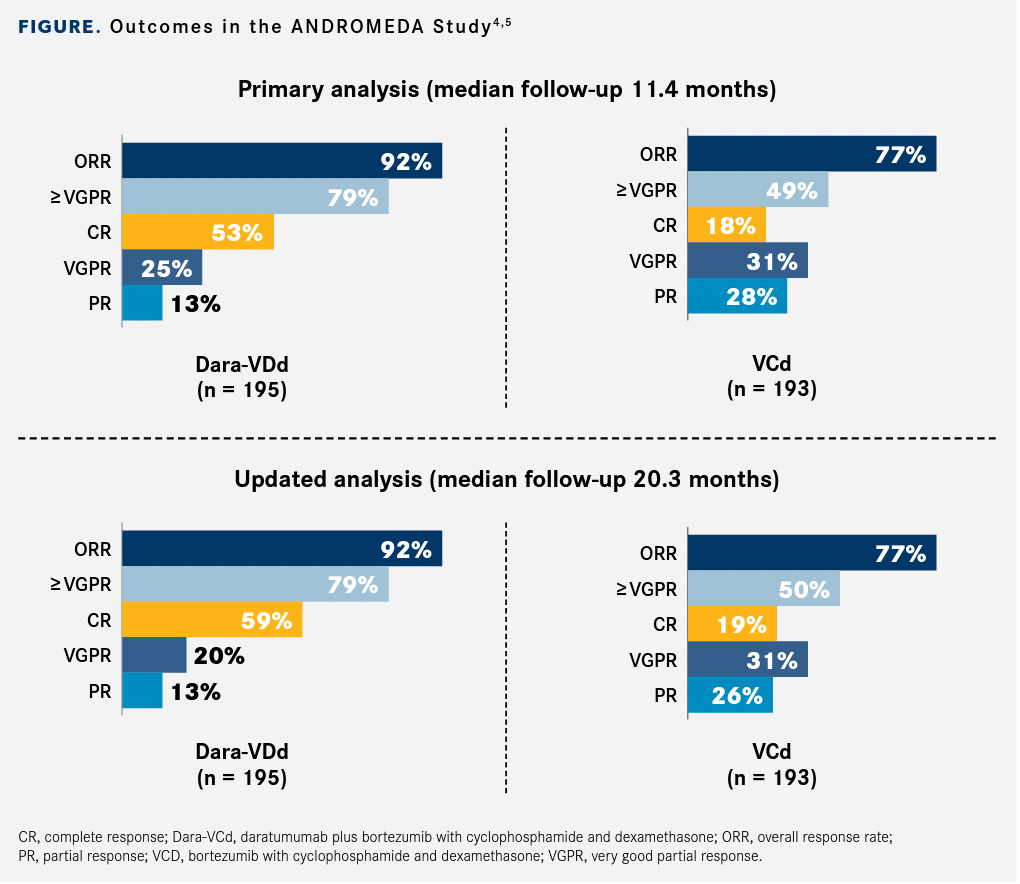
Patients were randomized to 6 cycles of VCd with or without daratumumab and hyaluronidase human-fihj (Darzalex Faspro) followed by maintenance Dara for 2 years in the Dara arm. The primary end point was overall complete hematologic response (CR) rate. Major organ deterioration progression-free survival (MOD-PFS) was a secondary end point which was a composite end point that included end-stage renal or cardiac failure, hematologic progression, and death. The study enrolled 338 patients with the majority having cardiac involvement (71%) and over a third having advanced cardiac disease (stage IIIA, 36%). After a median follow-up of 11.4 months, the results were intriguing. More than half of patients who received Dara-VCd (n = 195) achieved hematologic CR (53%; 95% CI, 46.1%-60.0%) vs 18% (95% CI, 13.0%-24.3%) of those who received VCd alone (n = 193; odds ratio [OR], 5.1; 95% CI, 3.2-8.2; P < .001).4
Additionally, the deep responses occurred rapidly with a median time to CR of 60 vs 85 days, respectively. These results were confirmed in an update presented at 2021 American Society of Clinical Oncology Annual Meeting5 (FIGURE4,5). The 6-month organ responses doubled with the quadruplet regimen (cardiac, 42% vs 22%; and renal, 53% vs 24%). The MOD-PFS composite end point was significantly better in the quadruplet arm (HR, 0.58) and the median time to next treatment was not reached vs 10.4 months in the VCd arm. Longer follow-up is needed for OS data to mature.4
All the adverse events (AEs) seen in this study were in line with prior experience with VCd and Dara. Serious adverse events occurred more frequently in the quadruplet arm (43%) vs 36% in the VCd arm but treatment discontinuation was a rare occurrence (4% in both arms). AEs also tended to abate once patients were switched to maintenance Dara. Dara administration–related reactions occurred in only 7% of the patients and were of low grade.4
What's Next for Amyloidosis
The results of the ANDROMEDA study supported the FDA approval of the quadruplet of Dara-VCd for the treatment of AL amyloidosis in January 2021 which constitutes the first FDA approval for this patient population. An ongoing phase 2 study (NCT04131309) is examining the role of Dara monotherapy in patients with stage IIIB AL amyloidosis who were excluded from ANDROMEDA.
Organ responses in AL amyloidosis tend to be slow with a median time to response of 10.4 months and many patients continue with irreversible organ damage and poor quality of life despite achieving a deep hematologic response.6 Thus, targeting the amyloid fibril has been the focus of clinical trials in order to restore organ function and improve prognosis.
Birtamimab (NEOD001) is a first in class humanized IgG1 which ensures clearance of deposited amyloid fibrils by phagocytosis. It showed improved organ responses in initial studies, but further development was interrupted in 2018 after the phase 2b PRONTO study (NCT02632786) did not meet its primary and secondary end points.7 Post hoc analyses of the randomized, double-blinded, placebo-controlled phase 3 VITAL study (NCT02312206) later found survival benefit for patients with advanced Mayo stage IV AL amyloidosis who received the study drug, leading to the return of birtamimab. The phase 3 AFFIRM-AL (NCT04973137) study is currently enrolling patients with Mayo stage IV AL amyloidosis.
CAEL-101 (11-1F4) is an amyloid-fibril reactive IgG1 monoclonal antibody that was found to be efficacious and without significant toxicity in the initial phase 1 study.8 The phase 2 dose selection study conducted at our center confirmed the safety profile of CAEL-101 and reported organ responses in all evaluable patients with renal AL amyloidosis. It also recommended 1000 mg/m2 as the phase 3 dose in combination with VCd.9 Updated organ responses in 18 patients were presented at the 63rd American Society of Hematology annual Meeting and Exposition and also included patients who received Dara in combination with VCd. The results were intriguing with organ responses seen in all 9 evaluable patients with renal involvement and 6 of 11 evaluable patients with cardiac involvement.10 Two ongoing randomized phase 3 studies are studying CAEL-101 in advanced AL amyloidosis (stages IIIA and IIIB) in combination with plasma-cell directed therapy (NCT04512235, NCT04504825).
We are seeing an unprecedented progress in the treatment of AL amyloidosis. Given the marked improvement in hematologic responses seen with the implementation of frontline daratumumab, the role of AHCT needs to be redefined especially its utility and timing. Anti-amyloid therapies are emerging as promising options to reverse organ damage and improve patients’ survival and quality of life. They will likely be included in the treatment paradigm of AL amyloidosis as clinical data continue to mature.
Reference
Palladini G, Dispenzieri A, Gertz MA, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes. J Clin Oncol. 2012;30(36):45414549. doi:10.1200/JCO.2011.37.7614
Kaufman GP, Schrier SL, Lafayette RA, Arai S, Witteles RM, Liedtke M. Daratumumab yields rapid and deep hematologic responses in patients with heavily pretreated AL amyloidosis. Blood. 2017;130(7):900-902. doi:10.1182/ blood-2017-01-763599
Khouri J, Kin A, Thapa B, et al. Daratumumab proves safe and highly effective in AL amyloidosis. Br J Haematol. 2019;185(2):342-344. doi:10.1111/bjh.15455
Kastritis E, Palladini G, Minnema MC, et al; ANDROMEDA Trial Investigators. Daratumumab-based treatment for immunoglobulin light-chain amyloidosis. N Engl J Med. 2021;385(1):46-58. doi:10.1056/NEJMoa2028631
Kastritis E, Sanchorawala Vm Merlini G, et al; ANDROMEDA Study Group. Subcutaneous daratumumab + bortezomib, cyclophosphamide, and dexamethasone (VCd) in patients with newly diagnosed light chain (AL) amyloidosis: updated results from the phase 3 ANDROMEDA study. J Clin Oncol. 2021;39(suppl 15):8003. doi:10.1200/JCO.2021.39.15_suppl.8003
Kaufman GP, Dispenzieri A, Gertz MA, et al. Kinetics of organ response and survival following normalization of the serum free light chain ratio in AL amyloidosis. Am J Hematol. 2015;90(3):181186. doi:10.1002/ajh.23898
Gertz MA, Landau H, Comenzo RL, et al. First-in-human phase I/II study of NEOD001 in patients with light chain amyloidosis and persistent organ dysfunction. J Clin Oncol. 2016;34(10):1097103. doi:10.1200/JCO.2015.63.6530
Edwards CV, Gould J, Langer AL, et al. Interim analysis of the phase 1a/b study of chimeric fibril-reactive monoclonal antibody 11-1F4 in patients with AL amyloidosis. Amyloid. 2017;24(suppl 1):58-59. doi:10.1080/13506129.2017.1292900
Khouri J, Anwer F, Samara CJ, et al. Safety, tolerability and efficacy of Cael-101 in AL amyloidosis patients treated on a phase 2, open-label, dose selection study to evaluate the safety and tolerability of Cael-101 in patients with AL amyloidosis. Blood. 2020;136(suppl 1):21. doi:10.1182/blood-2020-137235
Valent J, Silowsky J, Kurman MR, et al. Updated organ response results of an open-label study to evaluate the safety and tolerability of Cael-101 in patients with AL amyloidosis receiving anti-plasma cell therapy. Blood. 2021;138(suppl 1):2724. doi:10.1182/ blood-2021-148905
https://www.onclive.com/view/unprecedented-advances-fuel-progress-in-the-treatment-of-al-amyloidosis
Disclaimer:《Unprecedented Advances Fuel Progress in the Treatment of AL Amyloidosis》Edited and sorted by Seagull Pharmacy's editors. Please contact us in time if there is any infringement. In addition, the suggestions for drug usage, dosage and disease mentioned in the article are only for medical staff's reference, and can not be used as any basis for medication!